Kenalog Lotion: Package Insert / Prescribing Info
Package insert / product label
Generic name: triamcinolone acetonide
Dosage form: Lotion USP
Drug class: Topical steroids
Medically reviewed by Drugs.com. Last updated on Mar 25, 2024.
On This Page
Kenalog Lotion Description
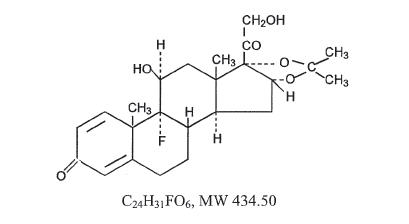
The topical corticosteroids constitute a class of primarily synthetic steroids used as anti-inflammatory and antipruric agents. The steroids in this class include triamcinolone acetonide. Triamcinolone acetonide is designated chemically as 9-Fluoro-11β, 16α, 17,21-tetrahydroxypregna-1,4-diene-3,20-dione cyclic 16,17-acetal with acetone. Graphic formula:
Each mL of 0.025% and 0.1% Kenalog Lotion (Triamcinolone Acetonide Lotion) provides 0.25 mg and 1 mg triamcinolone acetonide, respectively, in a lotion base containing propylene glycol, cetyl alcohol, stearyl alcohol, sorbitan monopalmitate, polysorbate 20, simethicone, and purified water.
Kenalog Lotion - Clinical Pharmacology
Topical corticosteroids share anti-inflammatory, antipruritic and vasoconstrictive actions.
The mechanism of anti-inflammatory activity of the topical corticosteroids is unclear.
Various laboratory methods, including vasoconstrictor assays are used to compare and predict potencies and/or clinical efficacies of the topical corticosteroids. There is some evidence to suggest that a recognizable correlation exists between vasoconstrictor potency and therapeutic efficacy in man.
Pharmacokinetics
The extent of percutaneous absorption of topical corticosteroids is determined by many factors including the vehicle, the integrity of the epidermal barrier, and the use of occlusive dressings.
Topical corticosteroids can be absorbed from normal intact skin. Inflammation and/or other disease processes in the skin increase percutaneous absorption. Occlusive dressings substantially increase the percutaneous absorption of topical corticosteroids. Thus, occlusive dressings may be a valuable therapeutic adjunct for treatment of resistant dermatoses (see DOSAGE AND ADMINISTRATION).
Once absorbed through the skin, topical corticosteroids are handled through pharmacokinetic pathways similar to systemically administered corticosteroids. Corticosteroids are bound to plasma proteins in varying degrees. Corticosteroids are metabolized primarily in the liver and are then excreted by the kidneys. Some of the topical corticosteroids and their metabolites are also excreted into the bile.
Indications and Usage for Kenalog Lotion
Kenalog Lotion (Triamcinolone Acetonide Lotion) 0.025% and 0.1% are indicated for the relief of the inflammatory and pruritic manifestations of corticosteroid-responsive dermatoses.
Contraindications
Topical corticosteroids are contraindicated in those patients with a history of hypersensitivity to any of the components of the preparations.
Precautions
General
Systemic absorption of topical corticosteroids has produced reversible hypothalamic-pituitary-adrenal (HPA) axis suppression, manifestations of Cushing’s syndrome, hyperglycemia, and glucosuria in some patients.
Conditions which augment systemic absorption include the application of the more potent steroids, use over large surface areas, prolonged use, and the addition of occlusive dressings.
Therefore, patients receiving a large dose of any potent topical steroid applied to a large surface area or under an occlusive dressing should be evaluated periodically for evidence of HPA axis suppression by using the urinary free cortisol and ACTH stimulation tests, and for impairment of thermal homeostasis. If HPA axis suppression of elevation of the body temperature occurs, an attempt should be made to withdraw the drug, to reduce the frequency of application, substitute a less potent steroid, or use a sequential approach when utilizing the occlusive technique.
Recovery of HPA axis function and thermal homeostasis are generally prompt and complete upon discontinuation of the drug. Infrequently, signs and symptoms of steroid withdrawal may occur, requiring supplemental systemic corticosteroids. Occasionally, a patient may develop a sensitivity reaction to a particular occlusive dressing material or adhesive and a substitute material may be necessary.
Children may absorb proportionally larger amounts of topical corticosteroids and thus be more susceptible to systemic toxicity (see PRECAUTIONS, Pediatric Use).
If irritation develops, topical corticosteroids should be discontinued and appropriate therapy instituted.
In the presence of dermatological infections, the use of an appropriate antifungal or antibacterial agent should be instituted. If a favorable response does not occur promptly, the corticosteroid should be discontinued until the infection has been adequately controlled.
These preparations are not for ophthalmic use.
Information for the Patient
Patients using topical corticosteroids should receive the following information and instructions:
- This medication is to be used as directed by the physician. It is for external use only. Avoid contact with the eyes.
- Patients should be advised not to use this medication for any disorder other than for which it was prescribed.
- The treated skin area should not be bandaged or otherwise covered or wrapped as to be occlusive unless directed by the physician.
- Patients should report any signs of local adverse reactions especially under occlusive dressing.
- Parents of pediatric patients should be advised not to use tight-fitting diapers or plastic pants on a child being treated in the diaper area, as these garments may constitute occlusive dressings.
Laboratory Tests
A urinary free cortisol test and ACTH stimulation test may be helpful in evaluating HPA axis suppression.
Carcinogenesis, Mutagenesis, and Impairment of Fertility
Long-term animal studies have not been performed to evaluate the carcinogenic potential or the effect on fertility of topical corticosteroids.
Studies to determine mutagenicity with prednisolone and hydrocortisone showed negative results.
Pregnancy
Teratogenic Effects
Category C. Corticosteroids are generally teratogenic in laboratory animals when administered systemically at relatively low dosage levels. The more potent corticosteroids have been shown to be teratogenic after dermal application in laboratory animals. There are no adequate and well-controlled studies in pregnant women on teratogenic effects from topically applied corticosteroids. Therefore, topical corticosteroids should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Drugs of this class should not be used extensively on pregnant patients, in large amounts, or for prolonged periods of time.
Nursing Mothers
It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in breast milk. Systemically administered corticosteroids are secreted into breast milk in quantities not likely to have a deleterious effect on the infant. Nevertheless, caution should be exercised when topical corticosteroids are administered to a nursing woman.
Pediatric Use
Pediatric patients may demonstrate greater susceptibility to topical corticosteroid-induced HPA axis suppression and Cushing’s syndrome than mature patients because of a larger skin surface area to body weight ratio.
HPA axis suppression, Cushing’s syndrome, and intracranial hypertension have been reported in children receiving topical corticosteroids. Manifestations of adrenal suppression in children include linear growth retardation, delayed weight gain, low plasma cortisol levels, and absence of response to ACTH stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema.
Administration of topical corticosteroids to children should be limited to the least amount compatible with an effective therapeutic regimen. Chronic corticosteroid therapy may interfere with the growth and development of children.
Adverse Reactions/Side Effects
The following local adverse reactions are reported infrequently with topical corticosteroids, but may occur more frequently with the use of occlusive dressings (reactions are listed in an approximate decreasing order of occurrence): burning, itching, irritation, dryness, folliculitis, hypertrichosis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, maceration of the skin, secondary infection, skin atrophy, striae, and miliaria.
Overdosage
Topically applied corticosteroids can be absorbed in sufficient amounts to produce systemic effects (see PRECAUTIONS, General).
Kenalog Lotion Dosage and Administration
Apply the 0.025% Kenalog Lotion (Triamcinolone Acetonide Lotion) to the affected area two to four times daily. Rub in gently.
Apply the 0.1% Kenalog Lotion (Triamcinolone Acetonide Lotion) to the affected area two to three times daily. Rub in gently.
Occlusive Dressing Technique
Occlusive dressings may be used for the management of psoriasis or other recalcitrant conditions. Gently rub a small amount of lotion into the lesion until it disappears. Reapply the the preparation leaving a thin coating on the lesion, cover with pliable nonporous film, and seal the edges. If needed, additional moisture may be provided by covering the lesion with a dampened clean cotton cloth before the nonporous film is applied or by briefly wetting the affected area with water immediately prior to applying the medication. The frequency of changing dressings is best determined on an individual basis. It may be convenient to apply Kenalog lotion under an occlusive dressing in the evening and to remove the dressing in the morning (i.e., 12-hour occlusion). When utilizing the 12-hour occlusion regimen, additional lotion should be applied, without occlusion, during the day. Reapplication is essential at each dressing change.
If an infection develops, the use of occlusive dressings should be discontinued and appropriate antimicrobial therapy instituted.
| KENALOG
triamcinolone acetonide lotion |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| KENALOG
triamcinolone acetonide lotion |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Bristol-Myers Squibb Company |
More about triamcinolone topical
- Check interactions
- Compare alternatives
- Pricing & coupons
- Reviews (105)
- Drug images
- Side effects
- Dosage information
- During pregnancy
- Drug class: topical steroids
- Breastfeeding
Patient resources
Professional resources
- Triamcinolone Acetonide (Topical) monograph
- Triamcinolone (FDA)
- Triamcinolone Lotion (FDA)
- Triamcinolone Ointment (FDA)
- Triamcinolone Paste (FDA)
Other brands
Trianex, Triderm, Oralone, DermacinRx Trizapak, ... +7 more